| Muscle | Origin | Insertion | Innervation | Action |
|---|---|---|---|---|
| Infraspinatus | Infraspinous Fossa of Scapula | Greater tubercle of Humerus | Suprascapular n. C4 - C6 |
GHJ: ER, Stabilization |
| Supraspinatus | Supraspinous Fossa of scapula | Greater tubercle of Humerus | Suprascapular n. C4 - C6 |
GHJ: Initiates abduction, Stabilization |
Suprascapular nerve

Anatomy
Origin
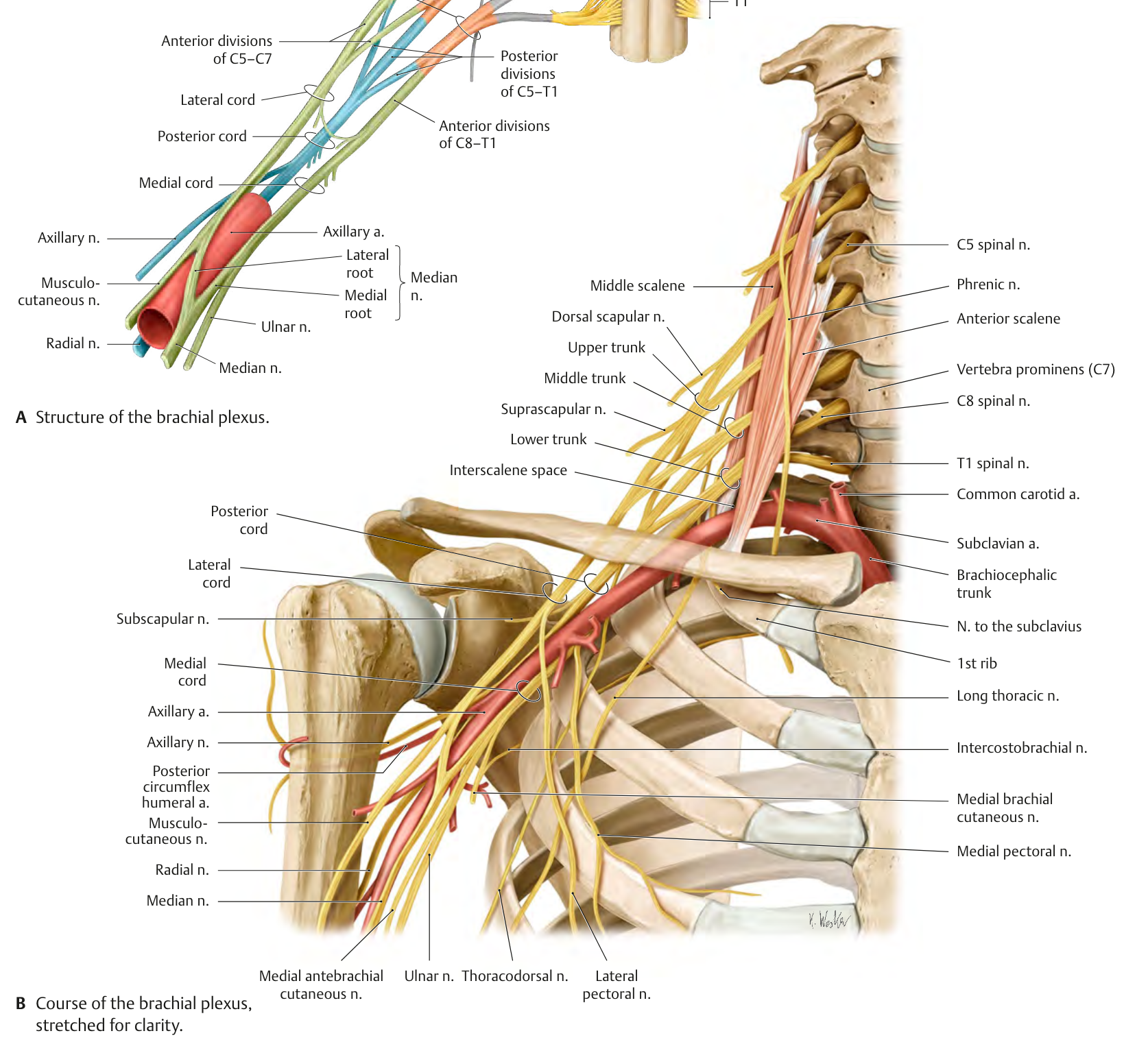
The suprascapular nerve originates from nerve roots C5, C6 via the Superior Trunk at Erb’s point2.
Path
The suprascapular nerve comes off the Superior Trunk and travels inferiorly and laterally posterior to the brachial plexus, parallel to the omohyoid muscle, and inferior to the trapezius to the superior edge of the scapula then through the suprascapular notch2. The suprascapular artery and vein initially run with the suprascapular nerve, but deviate and run superior to the transverse suprascapular ligament over the suprascapular notch2.
Termination
- After passing through the notch, the nerve supplies motor innervation to the supraspinatus muscle2.
- The nerve also gives off afferent articular branches to the GHJ and ACJ1,2.
- The suprascapular nerve then passes inferiorly to the scapular spine via the spinoglenoid notch to provide motor innervation to the infraspinatus muscle1,2.
Motor Innervation
Joint innervation
Cutaneous Innervation
The suprascapular nerve has cutaneous branches, which provide sensation to the proximal \(\frac{1}{3}\) of the arm, but their distribution overlaps with that of the supraclavicular and axillary nerves2.
Examination
- Empty can / Jobe test can be used to determine suprascapular nerve integrity by testing supraspinatus muscle
Injury
Compression, traction, or laceration can all cause injury to the suprascapular nerve2.
Compression Injury
A direct trauma at Erb’s point can cause a compression-type injury2. Compression neuropathy of the suprascapular nerve commonly occurs at the scapular notch under the transverse scapular ligament or at the spinoglenoid notch2. Compression at either of these notches occurs through extraneural inflammation, lipoma or cyst development, scarring following distal clavicle resection, or ligament entrapment2. Ligament entrapment can be caused from an acute trauma resulting from a fall on an outstretched hand (FOOSH), scapular fracture, or overuse injuries due to repetitive overhead motions2.
Important
Entrapment of the suprascapular nerve is easily misdiagnosed as rotator cuff tendinitis, RTC tear, or cervical disk disease2
Clinical Presentation
Pain due to suprascapular nerve entrapment can radiate to the lateral neck or posterior and lateral aspects of the glenohumeral joint capsule2.
As the suprascapular nerve is a mixed nerve, the patient presentation can include motor and sensory symptoms:
- A dull, deep ache at the posterior and lateral aspects of the shoulder, which may have a burning quality2
- Muscle atrophy and weakness of the supraspinatus and infraspinatus2
- Compensatory GHJ changes due to supraspinatus weakness, such as increased scapular elevation during arm elevation2.
- This may produce impingement-like findings and complicate the diagnosis2
- Full external rotation of the G-H joint and passive horizontal adduction are painful2
Intervention
Conservative
“Conservative intervention includes rest, ice, analgesics, and a series of perineural injections of corticosteroid to help reduce neural inflammation. A home exercise program of scapular pivoter strengthening (see Chapter 16), scapulohumeral coordination exercises (see Chapter 16), and activity-specific training may be indicated”2
Surgical
“Surgical intervention, involving neurolysis, cyst removal, or the excision of the transverse scapular ligament is indicated if symptoms persist”2
Entrapment
References
1.
Gilroy AM, MacPherson BR, Wikenheiser JC, Voll MM, Wesker K, Schünke M, eds. Atlas of Anatomy. 4th ed. Thieme; 2020.
2.
Dutton M. Dutton’s Orthopaedic Examination, Evaluation, and Intervention. 5th ed. McGraw Hill Education; 2020.
3.
Kolar P. Clinical Rehabilitation. 1st ed. Dynamic Neurological Stabilization; 2014.
Citation
For attribution, please cite this work as:
Yomogida N, Kerstein C. Suprascapular nerve. https://yomokerst.com/The
Archive/Anatomy/Nerves/Upper extremity
nerves/suprascapular_nerve.html